Running a 50–200 rep field force on Excel and WhatsApp is not a cost saving — it is a visibility tax. By the time the data reaches you, the month is already half gone. You are not managing your field force. You are auditing it, after the fact, when nothing can be changed. Every medical representative app, MR app, or field force management software promises to solve this — but choosing the wrong one costs you more than the Excel it replaces. The Indian pharma market is at a digital inflection point — the companies building field force intelligence today will be significantly harder to displace in three to five years. This guide tells you exactly what to look for, what to avoid, and how to evaluate before you commit. No jargon, no vendor hype — just the questions a CEO should ask before signing any medical representative software contract.
01. The invisible problem with Excel and WhatsApp
Most CEOs of mid-size Indian pharma companies know their field force reporting is imperfect. What they underestimate is how expensive that imperfection actually is.
The signs are familiar. DCA targets are missed — but you find out at the month-end review, not on Day 12 when there are still 13 days left to recover. Your MRs fill their Daily Call Reports from memory at 9pm, not from the field at 11am. You have no idea which doctors are being visited consistently and which are being quietly skipped. Expense claims arrive in a pile and someone spends three days reconciling them. RCPA data exists — somewhere — but it is never properly analysed.
None of these feel like crises. They feel like the cost of doing business. But they are not — they are the cost of not having visibility. And that cost compounds, territory by territory, month after month, in ways that only become visible when a competitor gains share and nobody can explain why.
"Stage 1 companies find out what went wrong at the month-end review. Stage 3 companies find out what is going wrong on Day 9 — when there are still 21 days left to fix it."
02. The Field Force Maturity Model — where are you today?
Before evaluating any SFA tool, it helps to understand where your field force stands today. Most Indian pharma companies with 100–200 reps sit in one of three stages.
Blind
"I find out what happened last month at the month-end review."
- DCRs filled from memory at end of day
- DCA targets missed — discovered too late
- No visibility of doctor visit patterns
- RCPA on paper, never analysed
- Expense claims manual and disputed
- Manager decisions made on instinct
Aware
"I know what my team did yesterday — but not what they are doing right now."
- Basic SFA in place — activity tracked
- Some visibility — but gaps remain
- Visits logged but not geo-verified
- DCA monitored but recovery too late
- Expensing partially improved
- No prescription intelligence
Intelligent
"I know what my team is doing right now — and which territories need my attention today."
- Geo-tagged visits, zero reporting lag
- DCA validated against targets mid-cycle
- RCPA collected and analysed
- Auto expensing — no forms, no disputes
- e-Detailing with engagement analytics
- Route optimised — more face time
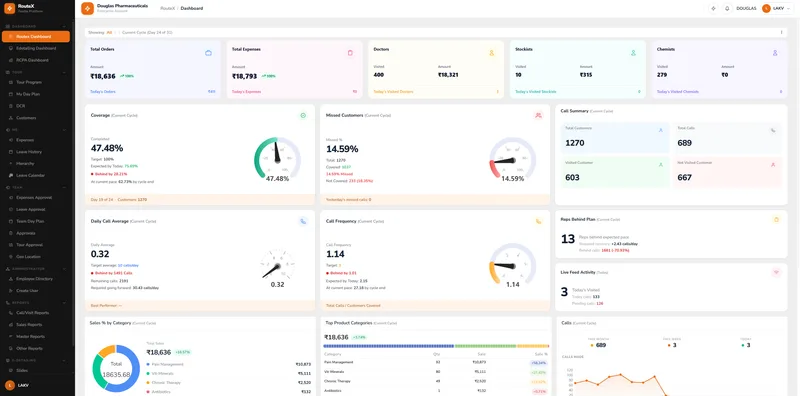
Most Indian pharma companies with 100–200 reps are still operating at Stage 1 — month-end visibility, manual reporting, and no way to verify what actually happened in the field. If you want to see what real-time field force intelligence looks like, we can show you the RouteX dashboard using a sample territory structure similar to yours.
See the RouteX dashboard →03. The real cost of staying at Stage 1
The pain of a Stage 1 field force is rarely felt as "poor DCA compliance." It is felt as flat territory numbers, a competitor gaining share in a district you thought was solid, or a doctor who used to write your brand and quietly stopped.
The root cause is almost always the same — you cannot manage what you cannot verify.
Without geo-tagged visit verification, you have no way of knowing how many of your logged visits actually happened. Industry experience with field forces on manual reporting systems suggests MRs consistently over-report visit activity — not always out of dishonesty, but because end-of-day DCR forms filled from memory are inherently unreliable. A visit that was cut short becomes a completed visit. A doctor who was unavailable becomes a visit that happened. Over a month, across a team of 100 MRs, the gap between reported activity and actual activity compounds in ways that only become visible when territory performance starts to slide.
| MRs logging visits per day | 50 MRs |
| Reported visits per MR per day | 10 visits |
| Total reported visits per month (× 25 days) | 12,500 visits |
| Estimated ghost visit rate on manual systems | 15–20% |
| Ghost visits per month (midpoint 17.5%) | ~2,188 |
| Ghost visits per MR per month | ~44 |
| Each ghost visit is a doctor logged as visited — but not seen | ~2,188 / month |
Based on industry experience with field forces transitioning from manual to geo-tagged digital reporting. These are not visits that definitively did not happen — some did. But without verification, you cannot know which ones. Every metric downstream of the visit log is only as reliable as the visit log itself.
These are not visits that did not happen — some did. But the doctor relationships you believe are being maintained may not be. A competitor who is showing up consistently to those same doctors is building the relationship you think you already have.
"Every metric downstream of the visit log is only as reliable as the visit log itself. If the log is built on memory, so is your territory intelligence."
Now here is what those ghost visits actually cost — in prescription revenue. Use your own numbers.
—
—
—
All inputs are adjustable — defaults are deliberately conservative. Ghost visit rate fixed at 17.5% (midpoint of 15–20%). Competitor switching risk of 50% based on published detailing frequency research showing significant prescription drift after 2 or more consecutive missed visit cycles.
These are not visits that did not happen — some did. But the doctor relationships you believe are being maintained, because your DCR shows they were visited, may not be. A competitor who is showing up consistently to those same doctors is building the relationship you think you already have.
"Every metric downstream of the visit log is only as reliable as the visit log itself. If the log is built on memory, so is your territory intelligence."
This is not a field force discipline problem. It is a data integrity problem — and it is one that only geo-tagged, real-time visit verification can solve.
04. 10 things every pharma SFA tool must do for Indian field forces
Use this as your evaluation checklist for any SFA tool — including Zoulte RouteX. If a tool cannot do all ten of these things well, it will not get you to Stage 3.
What every MR app for Indian pharma must include
Whether you are evaluating a dedicated medical representative app or a broader field force management software platform, the feature checklist below separates tools that are genuinely built for Indian pharma from those that merely claim to be.
Real-time DCA tracking with target validation
Not just logging calls — flagging when a rep falls behind mid-cycle so recovery is still possible. The difference between knowing on Day 15 and knowing on Day 28 is the difference between fixing the problem and writing it off.
Geo-tagging of every visit
Visit verification that answers the question every manager has but rarely asks out loud: "Is my MR actually where they say they are?" Geo-tagging turns trust-based reporting into verified reporting.
Route planning and optimisation
An MR who spends 90 minutes travelling between visits instead of 30 is making 3 fewer calls per day. Over a 25-day cycle that is 75 missed visits per MR. Route optimisation is not a convenience feature — it is a DCA feature.
Doctor categorisation with visit targets per tier
Gold, Silver, Bronze — or whatever your company already calls them. Targets set per category. Achievement tracked in real time. Without this, every doctor is treated equally — which means your highest-value doctors are being under-served.
Tour planning built around the Indian DCA model
Daily patch planning, priority doctor scheduling, monthly cycle management. The tool must understand how Indian pharma territories actually work — not impose a generic CRM logic on a field force structure it was not built for.
RCPA collection at the point of visit
Chemist audits logged in the field, not reconstructed at the desk. If your MR is filling RCPA data from memory at the end of the day, it is not RCPA data — it is an educated guess.
Sample and gift tracking with compliance record
A complete, automatically maintained audit trail of samples distributed and gifts given. In a compliance-conscious environment, this protects the company — not just tracks the MR.
Auto expensing from actual field activity
Daily allowance triggered by verified geo-tagged presence. Travel expenses calculated from your uploaded distance and rate card table. No forms. No end-of-month pile. No disputes. The system calculates what happened because it tracked it in real time.
e-Detailing — offline capable, analytics when connected
Presentations that work in any clinic regardless of connectivity. When the MR reconnects, engagement data syncs automatically — so managers know not just that the detail happened, but how the doctor responded to it.
Manager dashboard with zero reporting lag
Live team visibility, DCA achievement by rep, missed visits, coverage tracking — right now, not at end of day. If the dashboard shows you yesterday, it is not a management tool. It is a history book.
05. Red flags in pharma SFA tools — what Indian buyers must watch out for
Most SFA tools will tell you they do everything on the checklist above. Here is how to tell whether they actually do.
Built for enterprise, priced for enterprise
Tools designed for 1,000-rep multinationals that have been re-skinned for mid-size teams. The complexity remains. The support does not.
Onboarding that takes weeks
If your MRs are not using the tool within days, adoption will never happen. Every week of delayed rollout is a week of continued Excel — and continued invisible losses.
Offline functionality buried in the fine print
Ask specifically: which features work offline and which require connectivity? Understand exactly what your MR can and cannot do without a signal before you sign.
End-of-day form filling disguised as real-time reporting
If the MR is still filling a DCR form at the end of the day, the tool has not solved the problem. It has digitised it. Ask to see exactly how a visit is logged — in the field, not at a desk.
Dashboards that show activity, not performance against targets
Knowing Rep A made 8 calls today is information. Knowing Rep A is behind their DCA target by 23 calls this cycle and needs 13 calls per day to recover is intelligence. Ask which one the dashboard shows.
Expense modules that still require manual input
"Automated expensing" that still needs the MR to enter amounts is not automated. Ask to see exactly how an expense is generated, approved and paid — start to finish.
Support that disappears after go-live
Ask specifically: what does ongoing support look like after the contract is signed? Who do I call on Day 47 when something breaks in the field?
06. Pharma SFA pricing in India — what is fair, what is a red flag
Pharma SFA tools are typically priced per user per month, billed annually. Three-tier pricing is the most common model — matching feature depth to the role using the tool.
| Tier | For | Core capabilities |
|---|---|---|
| Operate | The MR in the field | Visit logging, DCA tracking, geo-tagging, route planning, doctor categorisation, sample and gift tracking, order capture, leave application |
| Optimise | The field force manager | Everything in Operate, plus e-Detailing, RCPA collection, auto expensing, real-time manager dashboard, DCA target validation, team visibility |
| Dominate | CEO / Head of Sales | Everything in Optimise, plus RCPA analytics, e-Detailing analytics, multi-territory dashboards, AI-powered insights, priority support |
What should always be included — onboarding, training, product updates and standard support. If any of these are charged separately, ask why.
What to watch out for — hidden implementation fees, charges per report, data export costs, and features that appear in the demo but are only available at a higher tier than quoted.
The real cost comparison: For a team of 100 reps, a mid-tier SFA investment is typically less than the monthly salary cost of a single MR — with visibility across the entire field force in return. The question is not whether you can afford SFA. It is whether you can afford the ₹4.5 crore in lost prescriptions that comes with not having it.
Three tiers built for the Indian pharma field force
Zoulte RouteX is available in three tiers — Operate, Optimise and Dominate — priced per user per month and billed annually. Onboarding is included at all tiers. Full pricing is available at the link below.
07. How to evaluate a pharma SFA tool before you commit
The best SFA tool is not the one with the most features — it is the one your MRs actually use every single day. Here is how to evaluate for adoption, not just functionality.
- Evaluate on adoption likelihood, not feature count. The tool with 40 features that your MRs ignore is worth less than the tool with 12 features they use every day without being told to.
- Ask for a demo with your own data. Your territory structure, your doctor list, your distance table. A vendor who cannot demo on your data is selling you a generic product.
- Get 5 MRs to use it for one full working day. Not a training session — a real field day. Watch what confuses them. Watch what they skip. Watch what they naturally use without being told.
- Check the manager dashboard first. Open it and time yourself. If you cannot understand what it is telling you within 60 seconds, your field managers will not use it under pressure.
- Ask one question that reveals everything: "What does my MR's screen look like at 9am when they start their day?" The answer tells you whether the tool was built for the field or for the boardroom.
- Ask about the distance table setup. How long does it take to upload your rate card and territory distances? This is a one-time task but it determines how quickly auto expensing goes live.
- Ask what happens to your data if you leave. A vendor confident in their product gives you a clean answer. A vendor who deflects this question is telling you something important.
08. The Zoulte RouteX answer
Zoulte RouteX is built specifically for the Indian pharma field force — not adapted from a global CRM, not re-skinned enterprise software. It was designed around the realities of the Indian DCA model, the patch system, the chemist and stockist layer, and the daily workflow of an MR who needs a tool that works as fast as they move.
Here is what Zoulte RouteX delivers against the 10-point checklist:
- Zero reporting lag — field activity visible to managers in real time, not at end of day
- Geo-tagged visit verification — every doctor, chemist and stockist visit confirmed by location
- Route planning and optimisation — intelligent daily routing built into the MR's morning workflow
- Doctor categorisation with target tracking — Gold, Silver, Bronze or any naming your company uses, with visit targets set and tracked per tier
- DCA validation against targets — not just tracking calls, but flagging shortfalls mid-cycle with the recovery rate required
- RCPA collection at the chemist — logged in the field, in real time, not reconstructed at the desk
- Auto expensing — daily allowance triggered by verified field presence, travel expenses calculated from your uploaded rate card
- e-Detailing — fully offline — presentations that run in any clinic without connectivity, syncing engagement data automatically when reconnected
- Sample, gift and order capture — complete daily workflow in a single app
- Manager dashboard — live DCA achievement by rep, coverage progress, reps behind plan, missed visit alerts
Three tiers — Operate, Optimise and Dominate — each designed for a specific role in the field force. Most Heads of Sales start at Optimise. CEOs who want prescription intelligence and multi-territory visibility choose Dominate. Onboarding takes days, not weeks.
From Stage 1 to Stage 3 — in days, not months
Zoulte RouteX gives you the visibility, verification and intelligence your field force has been operating without. Real-time DCA tracking. Geo-tagged visits. RCPA collected at the chemist. Auto expensing. e-Detailing that works offline. All in one platform, built for India.
Questions about Zoulte RouteX?
Straight answers to what CEOs and Heads of Sales ask before signing.
Operate is the complete daily toolkit for the MR in the field — visit logging, DCA tracking, geo-tagging, route planning, doctor categorisation and order capture. Optimise adds the management and engagement layer — e-Detailing, RCPA collection, auto expensing and real-time team dashboards for the manager. Dominate adds the intelligence layer for the CEO or Head of Sales — RCPA analytics, e-Detailing analytics, multi-territory visibility and AI-powered insights.
See full tier comparison →The RouteX field app requires an active internet connection to log visits, geo-tag activity and update the manager dashboard in real time — which is the source of its zero reporting lag capability.
Zoulte's e-Detailing app, included in the Optimise tier, works fully offline. Presentations run without connectivity and sync engagement data automatically when the MR reconnects — so no detail visit is ever lost.
Learn more about e-Detailing →Territory setup — including doctor lists, chemist and stockist data, and doctor categorisation — is handled during onboarding with support from the Zoulte team. The distance table for auto expensing requires your existing rate card to be uploaded in a standard format.
Most companies complete the full setup within their first few days on the platform. You bring your existing territory structure and rate card — we automate it.
Talk to us about your setup →Zoulte RouteX is built to be field-ready fast. The interface is designed for MRs on the move — not for people sitting at a desk — so it is intuitive, fast and requires minimal training. Most teams are fully operational within days of signing up.
Onboarding support is included at all tiers. Managers have access to setup tools that make it straightforward to load territory data, doctor lists and product information quickly so the whole team can start together.
Request a Demo →Your data belongs to you. If you decide to leave Zoulte RouteX, your field activity data, doctor lists, RCPA records and reports are available for export before your account is closed. We do not hold your data hostage — and we are confident enough in the product that we do not need to.
Talk to our team →Ready to move from Stage 1 to Stage 3?
Zoulte RouteX gives your field force the visibility, verification and intelligence to stop losing ₹4.5 crore in prescriptions every year — and start building the kind of field force intelligence that compounds over time.
Built for India. Priced for 100–200 rep teams. Up and running in days.